




|We bring to you the very best in Pediatric Ophthalmology & Strabismus
There is a need of spreading more awareness among pediatricians and primary care physicians to recognise the common peditric eye diseases. They are the primary doctors of the child and anything missed at that level may present to the pediatric ophthalmologist very late, by which time the chances visual recovery may not be very good.
![]() Power is increasing rapidly!
Power is increasing rapidly!![]() Can increase in glass power be stopped?
Can increase in glass power be stopped?![]() Is myopia hereditary?
Is myopia hereditary?![]() Is squint only a cosmetic problem which can be ignored till the child grows up?
Is squint only a cosmetic problem which can be ignored till the child grows up?![]() Is Pediatric Cataract same as adult cataract?
Is Pediatric Cataract same as adult cataract?![]() Is Pediatric Cataract Surgery an elective surgery?
Is Pediatric Cataract Surgery an elective surgery?![]() Is Surgery alone enough for the child to gain maximum visual potential?
Is Surgery alone enough for the child to gain maximum visual potential?![]() Do premature children need routine eye check-up?
Do premature children need routine eye check-up?![]() If yes, when and why?
If yes, when and why?![]() What is ROP?
What is ROP?
If we are able to answer these questions correctly, then we will be in better equipped to realize the seriousness of some of the pediatric eye problems. With majority of the ophthalmologists too being very busy with their adult patients, the children were often deprived of proper attention. But then the realization came that if we compare the life expectancy of our pediatric patients, one blind child will be equivalent to 5 blind adults. This led to the evolution of Pediatric Ophthalmology as a separate sub-speciality.
Some important clues to suspect eye diseases in children are:
![]() Antenatal Infection – TORCH
Antenatal Infection – TORCH![]() Consanguinity
Consanguinity![]() Birth Trauma and Anoxia
Birth Trauma and Anoxia![]() Family History – Down Syndrome, Myopia, Squint, Retinal Detachment
Family History – Down Syndrome, Myopia, Squint, Retinal Detachment![]() Premature Delivery with Oxygen Therapy
Premature Delivery with Oxygen Therapy![]() Delayed Milestones
Delayed Milestones![]() Sibling involvement
Sibling involvement![]() Abnormal Eye Movements
Abnormal Eye Movements
Vision Assessment in Children:
A major hurdle in detecting eye problems is recording vision of infants and pre-school going children, where often they are not co-operate or not conversant to respond to instructions. However, at B B Eye Foundation, we train our optometrists particularly in vision assessment in children with modern and time tested instrumentation. Along with our Pediatric Ophthalmologists, we are able to diagnose and detect subtle childhood eye and vision problems. Some methods employed in the same are: .




|Visual Evoked Potential (VEP)
![]() Cortical potential have been used to assess visual acuity in children.
Cortical potential have been used to assess visual acuity in children.![]() VEP latency rather than amplitude is used to measure visual acuity.
VEP latency rather than amplitude is used to measure visual acuity.![]() It has been extremely helpful for collecting information on maturation of visual functions.
It has been extremely helpful for collecting information on maturation of visual functions.![]() Whether the responses from the two eyes differ is recorded.
Whether the responses from the two eyes differ is recorded.![]() Is used to chart progression of the condition in case of bilateral reduced visual acuity.
Is used to chart progression of the condition in case of bilateral reduced visual acuity.
|The most common pediatric eye diseases
Amblyopia (Lazy Eye)
Types
![]() Strabismic
Strabismic![]() Anisometropic (Best Prognosis)
Anisometropic (Best Prognosis)![]() Sensory Deprivation (Worst Prognosis)
Sensory Deprivation (Worst Prognosis)![]() Treatment done by proper optical correction and patching of the better eye.
Treatment done by proper optical correction and patching of the better eye.![]() Treatment of Amblyopia is possible only till a certain age.
Treatment of Amblyopia is possible only till a certain age.
Strabismus and sensory deprivation amblyopia (caused by media opacities like pediatric cataract, ptosis, lid hemangiomas etc) are easy to detect. It is important to recognise these conditions as serious enough to cause permanent visual impairment in children. Children with sensory deprivation amblyopia may require urgent surgical intervention before amblyopia therapy by glasses and patching is initiated.


|Strabismus (Squint)
![]() Infantile Esotropia
Infantile Esotropia![]() Accomodative Esotropia
Accomodative Esotropia![]() Intermittent Divergent Exotropia
Intermittent Divergent Exotropia![]() Paralytic Strabismuss Syndromes
Paralytic Strabismuss Syndromes
The first three are the most common and important in children. It is important to understand that squint is not just a cosmetic problem. It can lead to amblyopia of one of the eyes. Satisfactory treatment for amblyopia caused by strabismus is available only upto 9-10 years of age.
Infantile esotropia
![]() Age of onset: Infancy.
Age of onset: Infancy.![]() Large angle esotropia without high refractory error.
Large angle esotropia without high refractory error.![]() May be associated with dissociated vertical deviation.
May be associated with dissociated vertical deviation.

Infantile Esotropia
Accomodative Esotropia
![]() Age of onset – Around 3 years.
Age of onset – Around 3 years.![]() May/may not be associated with high hypermetropia.
May/may not be associated with high hypermetropia.![]() Generally gets corrected by optical correction.
Generally gets corrected by optical correction.![]() Bifocals to be given for high AC/A ratio.
Bifocals to be given for high AC/A ratio.![]() Early treatment important to prevent amblyopia.
Early treatment important to prevent amblyopia.

Accomodative Esotropia
Intermittent Divergent Squint
![]() Onset – infancy to early childhood.
Onset – infancy to early childhood.![]() Generally preserves fusion and stereopsis.
Generally preserves fusion and stereopsis.![]() Surgical results good.
Surgical results good.![]() Early detection of amblyopia if any, important.
Early detection of amblyopia if any, important.
Intermittent Divergent Squint
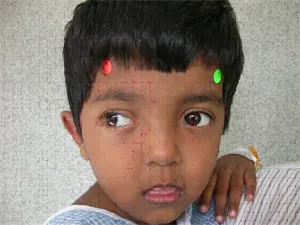
Squint in children can be detected by simple hirschberg test in which a torch light is shown to the child’s eye and the posittion of the corneal light reflex determined. Normally it should fall on the centre of the pupil in both eyes. If one of the reflex is on the centre of pupil and other peripherally, it indicates that the child is having squint.
|Squint – Take home message
![]() Not a cosmetic problem in children.
Not a cosmetic problem in children.![]() Needs immediate attention.
Needs immediate attention.![]() Can cause permanent visual impairment in one or both the eyes.
Can cause permanent visual impairment in one or both the eyes.![]() Early surgery may be necessary to maintain binocular vision and stereopsis.
Early surgery may be necessary to maintain binocular vision and stereopsis.![]() Can appear in adulthood as well – Mostly paralytic.
Can appear in adulthood as well – Mostly paralytic.![]() May need more than one surgery for full correction.
May need more than one surgery for full correction.![]() Has to be combined with amblyopia therapy to achieve best results.
Has to be combined with amblyopia therapy to achieve best results.![]() Routine follow up important.
Routine follow up important.![]() Squint may be the only clinical manifestation of Retinoblastoma.
Squint may be the only clinical manifestation of Retinoblastoma.
Nystagmus
It is almost anivariably associated with subnormal vision. Could be either sensory or congenital motor nystagmus. Any abnormality in the anterior visual pathway right from the cornea to optic tract can lead to nystagmus. But if such a pathology is not detected and nystagmus is present along with abnormal head posture, it is more likely to be a case of congenital motor nystagmus. In congenital motor nystagmus the binocular vision is generally good, and such children should not be encouraged to correct their head posture. It is an attempt to improve their vision by adopting a posture at which the nystagmus is least. The head posture alternatively can be corrected by surgery on the extraocular muscles. Latent nystagmus may be associated with infantile esotropia.
Congenital Cataract
![]() Dense unilateral cataract in children is considered an emergency and should be operated immediately.
Dense unilateral cataract in children is considered an emergency and should be operated immediately.![]() Even bilateral cataract should be operated as early as possible.
Even bilateral cataract should be operated as early as possible.![]() Sensory deprivation amblyopia caused by congenital cataract has worst prognosis if left unattended.
Sensory deprivation amblyopia caused by congenital cataract has worst prognosis if left unattended.![]() Rubella in 1st trimester may lead to total cataract.
Rubella in 1st trimester may lead to total cataract.![]() Amblyopia therapy following cataract surgery is as imporatant as the surgery itself.
Amblyopia therapy following cataract surgery is as imporatant as the surgery itself.


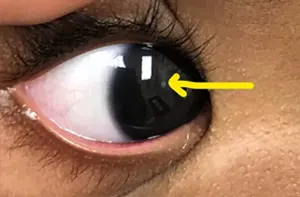
|White Pupillary Reflex
White Pupillary Reflex requires immediate attention because it could be both life threatening and cause permanent visual loss. The common causes of leucocoria are Congenital cataract, Other notable causes are:
![]() Retinoblastoma,
Retinoblastoma,![]() Retinopathy of prematurity,
Retinopathy of prematurity,![]() Coats disease,
Coats disease,![]() Toxocariasis,
Toxocariasis,![]() Primary hyperplastic persistent vitreous
Primary hyperplastic persistent vitreous

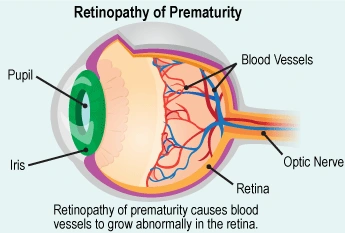
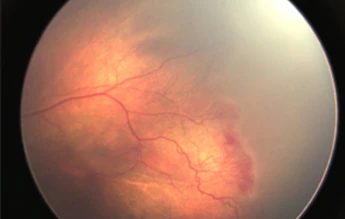
|Retinopathy of Prematurity (ROP)
![]() It is a bilateral disease that affects the vitreous and peripheral retina.
It is a bilateral disease that affects the vitreous and peripheral retina.![]() It is caused by a combination of factors, of which the most important is prematurity.
It is caused by a combination of factors, of which the most important is prematurity.![]() Increase in incidence is due to better neonatal care available in present hospitals resulting in better survival rate of premature children.
Increase in incidence is due to better neonatal care available in present hospitals resulting in better survival rate of premature children.![]() Timely treatment in early stage with laser may prevent irreversible visual loss.
Timely treatment in early stage with laser may prevent irreversible visual loss.
Risk Factors for ROP are:
![]() Prematurity
Prematurity![]() Low birth weight
Low birth weight![]() Complex neonatal hospital course
Complex neonatal hospital course![]() Prolonged supplimental oxygen
Prolonged supplimental oxygen
Screening Protocol
![]() Children born at less than 32 weeks of gestation or weighing less than 1500 gm, when they have reached age of 5 wks from birth or 32 weeks postconception (whichever is later).
Children born at less than 32 weeks of gestation or weighing less than 1500 gm, when they have reached age of 5 wks from birth or 32 weeks postconception (whichever is later).![]() If no ROP is found, then one more check after one month is required.
If no ROP is found, then one more check after one month is required.
|Retinoblastoma
![]() It is the most common intraocular malignancy of childhood.
It is the most common intraocular malignancy of childhood.![]() More than 90% of children can be cured of retinoblastoma by early detection and treatment of the affected eye.
More than 90% of children can be cured of retinoblastoma by early detection and treatment of the affected eye.![]() The average age of children with retinoblastoma is 18 months.
The average age of children with retinoblastoma is 18 months.![]() Most common presentation is white pupillary reflex.
Most common presentation is white pupillary reflex.

Treatment options available are:
![]() Laser therapy
Laser therapy![]() Cryotherapy
Cryotherapy![]() Brachytherapy
Brachytherapy![]() Chemotherapy
Chemotherapy![]() Enucleation
Enucleation
Examination of siblings is important
Buphthalmos
Salient features are:
![]() Large eyeball.
Large eyeball.![]() Bluish sclera.
Bluish sclera.![]() Child Photophobic.
Child Photophobic.![]() Sturge Weber Syndrome.
Sturge Weber Syndrome.
Early treatment necessary to preserve vision
![]() One should rule out infantile glaucoma if any child with large eyeballs and bluish tinge on the sclera is not able to tolerate light.
One should rule out infantile glaucoma if any child with large eyeballs and bluish tinge on the sclera is not able to tolerate light.
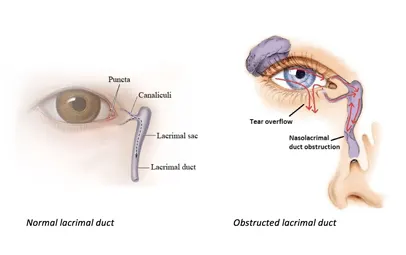
Infantile Nasolacrimal Duct Block
It is a common problem in infants which leads to mucoid discharge and watering from one or both the eyes. In most of the cases it can be treated by simple massage in the lacrimal sac area. Proper technique of massage is important. Most of the times patients don’t respond to treatment due to improper massage technique. It may lead to unnecessary syringing and probing under general anesthesia later on.
|Congenital Nasolacrimal Duct Block
It is a common problem in infants which leads to mucoid discharge and watering from one or both the eyes. In most of the cases it can be treated by simple massage in the lacrimal sac area. Proper technique of massage is important. Most of the times patients don’t respond to treatment due to improper massage technique. It may lead to unnecessary syringing and probing under general anesthesia later on.